Medical Mystery of the Week
Because of the COVID19 pandemic, you are practicing telemedicine. You interview a
45-year-old man who is complaining of periodic fevers, fatigue, and sleepiness. You
note that he appears to have enlargement of his cervical lymph nodes and that he has
a faint generalized maculopapular rash. An abdominal ultrasound performed several
days previously shows evidence of hepatospenomegaly. You are shown a photograph of
a slide of his peripheral blood (see below).
What is your diagnosis, what test(s) do you recommend to confirm your suspicions,
and what treatment, if any, do you recommend?
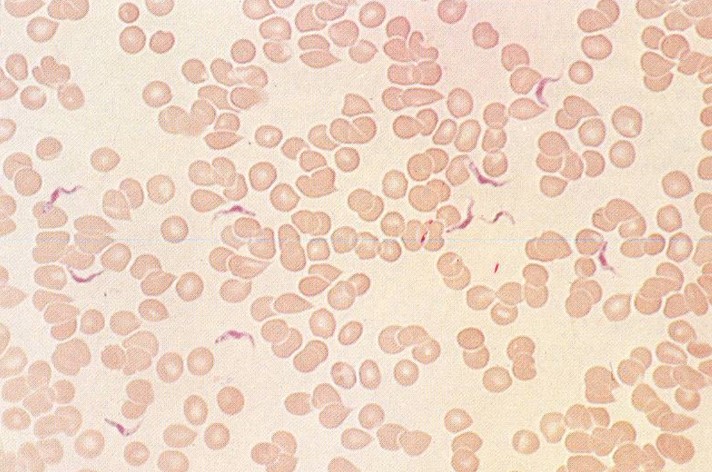
DIAGNOSIS: African trypanosomiasis due to infection with Trypanosoma brucei rhodesiense. T. b. rhodesiense accounts for ∼ 5% of human African trypanosomal infections and T. b. gambiense accounts for the remaining 95%. Early CNS involvement is more common with T. b. rhodesiense than with T. b. gambiense infection. Trypanosomiasis is usually transmitted by the bite of the tsetse fly although
it can be acquired via blood or plasma transfusion.
Once the cause of major epidemics in Africa, disease surveillance and treatment
programs have resulted in a significant decrease in clinically evident disease; however,
asymptomatic carriers remain a significant concern.
The clinical manifestations of African trypanosomiasis are diverse and vary
between travelers and persons endemic to the disease. For example, travelers are more
likely to present with GI manifestations such as diarrhea and jaundice than native
Africans. However, in both travelers and Africans, nonspecific symptoms and signs
are common and may include intermittent fever, malaise, arthragias, headache, lymphadenopathy,
hepatosplenomegaly, pericarditis and congestive heart failure.
Neurological manifestations of African trypanosomiasis are protean and may include
pyramidal and extrapyramidal signs, myelopathy, cerebellar ataxia, slurring of speech
and psychiatric disturbances. Classic signs of CNS involvement (daytime somnolence
and nocturnal insomnia) are more common with T. b. rhodesiense whereas Winterbottom's sign (posterior cervical adenopathy) is more common with T. b. gambiense infection. The pathways whereby trypanomsomes traverse the blood brain barrier (BBB)are
thought to include infection of microvascular neurophils and entry of the parasites
via fenestrated vessels in the choroid plexus and circumventricular regions.
The diagnosis of African trypanosomiasis is made by examination of thick/thin
blood smears which are more likely to be positive in T. b. rhodesiense infections. A card agglutination test is used extensively in endemic regions but the
test has a high incidence of false positive results. A rapid diagnostic test called
SD BIOLINE HAT recognizes two trypanosomal antigens (VSG Li'Tat 1.3 and VSG Li'Tat
1.5) and has a high sensitivity and specificity; it will detect all patients requiring
treatment.
Intravenous suramin is used to treat early-stage T. b. rhodesiense infection. Intravenous or intramuscular pentamidine is used to treat early stage T. b. gambiense infection. The only treatment currently available to treat late stage trypanosomiasis
is intravenous melarsoprol which, although effective, is very toxic with a fatality
rate of 5-9% due in large part to a post-treatment reactive encephalopathy thought
to be due to rapid parasite killing and the induction of a cytokine storm.
For an excellent review of human African trypansomias the Editor suggested reading
Kennedy, P.G.E.; Rodgers, J. Clinical and neuropathogenic aspects of human african
trypanosomiasis. 2019. Front. Immunol. 10:39. doi 10.3389/fimmun.2019.00039.